Background
What is Laparoscopic Sleeve Gastrectomy?
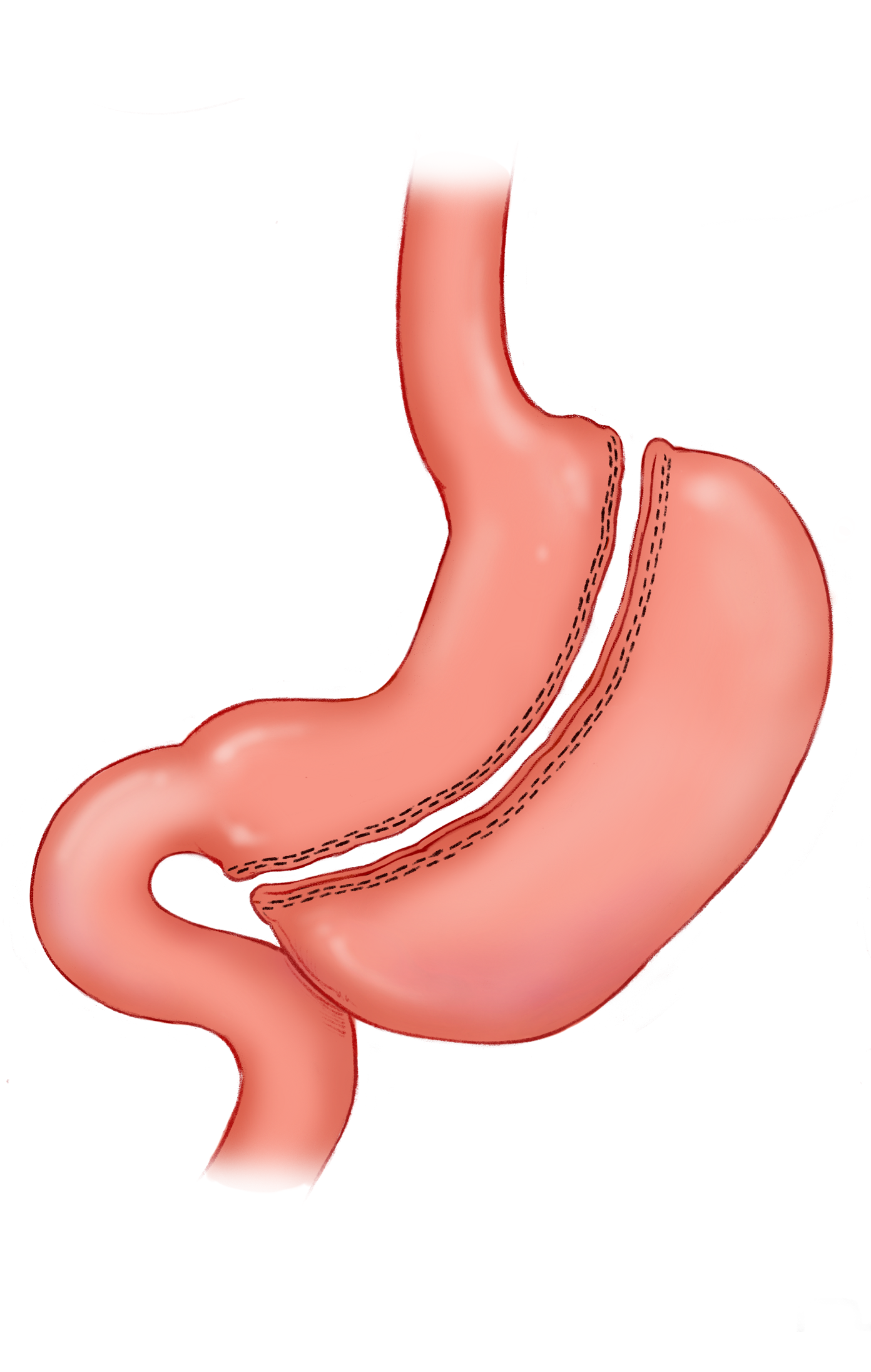
- Minimally invasive partial resection of the stomach along the greater curvature to create a sleeve or tubular morphology.
- Weight loss results due to restrictive and endocrine mechanisms
Indications
- Morbid obesity BMI >40
- Stand-alone treatment
- High-risk patients
- Kidney and liver transplant candidates
- Metabolic syndrome
- BMI 30-35 with comorbidities
Contraindications
- Barrett’s esophagus
- Some consider it an absolute contraindication due to future need for gastric-pull surgery with cancer.
- GERD (relative)
- Prohibitive anesthesia risk
- Uncontrolled psychiatric illness
- Coagulopathy
Operative Procedure
Laparoscopic
- Identify pylorus
- Mobilize greater curvature and ligate gastroepiploic and short gastric vasculature
- Assess hiatus for hernia
- Insert Bougie
- Transect stomach beginning 3-6 cm proximal to the pylorus
- Extract specimen
Advantages
- No enteric anastomosis
- No risk of internal hernia, dumping syndrome, or marginal hernia
- Decreases ghrelin
- Maintains access to pancreaticobiliary system
- Similar effect on weight loss
- Technically simpler
Normal Post Operative Appearance
What is Laparoscopic Sleeve Gastrectomy? CT Case Study 1 CT Case Study 2 Medical Illustration
- Minimally invasive partial resection of the stomach along the greater curvature to create a sleeve or tubular morphology.
- Weight loss results due to restrictive and endocrine mechanisms
Complications
Overall rate is less than gastric bypass
Leak- most common CT Case Study
- More susceptible to a leak than RYGB (2.4 versus 0.7%)
- Most often occurs at the proximal end
- Majority occur more than 10 days postop
- Imaging
- Contrast extravasation or opacification of a drain
- Free air or air fluid level adjacent to site of leak
- Staple line gap
- Phlegmon or abscess
Fistula CT Case Study
- Gastrocutaneous, gastrocolic, and gastrobronchial
- Imaging
- Contrast connection
- Fluid collection or abscess, effusion
Bleeding CT Case Study Medical Illustration
- Staple line, splenic Injury
- Imaging
- Fluid collection with high-density content or fluid-fluid level
- Contrast extravasation
Stricture CT Case Study Medical Illustration
- Acute or chronic
- Often occurs at incisura angularis
- Imaging- use MPRs
- Dilated proximal stomach and esophagus
- Luminal narrowing of stomach
- Contrast stasis proximally
- Angulation of stomach at stenosis
Portal Vein Thrombosis
- Rare
Splenic infarct- rare
- Related to ligation of short gastric vessels to mobilize fundus
- Imaging
- Wedge shaped peripheral area of hypodensity
Redundant gastric remnant
GERD
- Imaging
- Reflux of oral contrast
- Hiatal hernia
- Distended esophagus
Wound complications and trocar site hernia
{kind=link}
{kind=link}
{kind=link}